Milk Fever in Cattle: Causes, Symptoms, Treatment & Prevention
What Is Milk Fever?
Milk Fever is a metabolic disorder observed in high-yielding cows and buffaloes. This disease primarily occurs due to inadequate nutrition during pregnancy or a severe calcium deficiency (acute hypocalcemia) in the body immediately after calving.
This disease occurs only in female animals, as only they produce milk; it is not found in male animals.
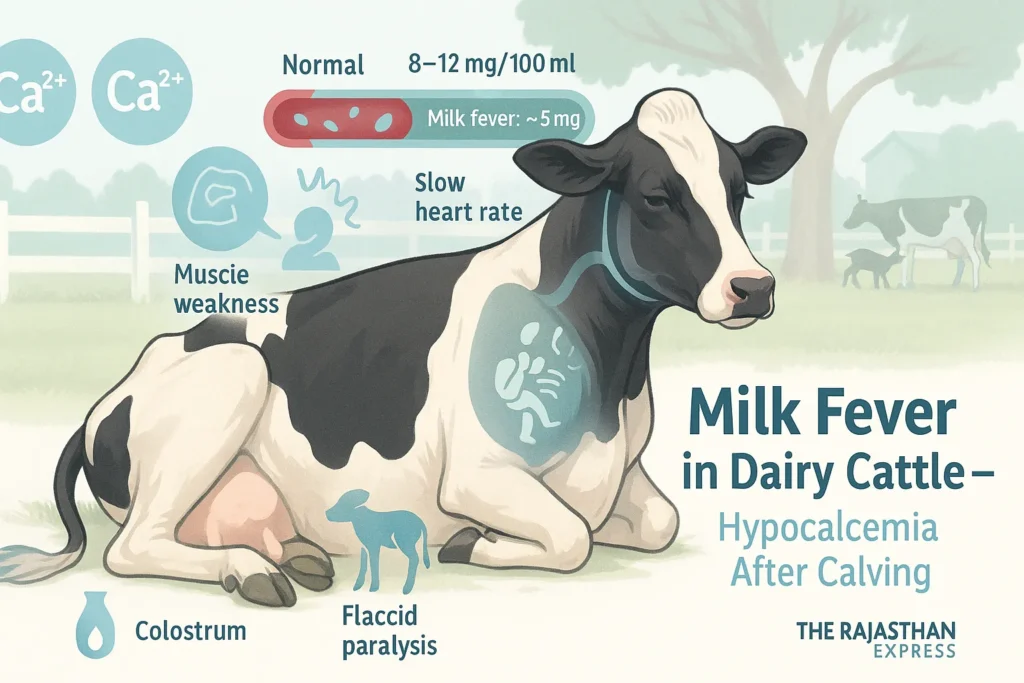
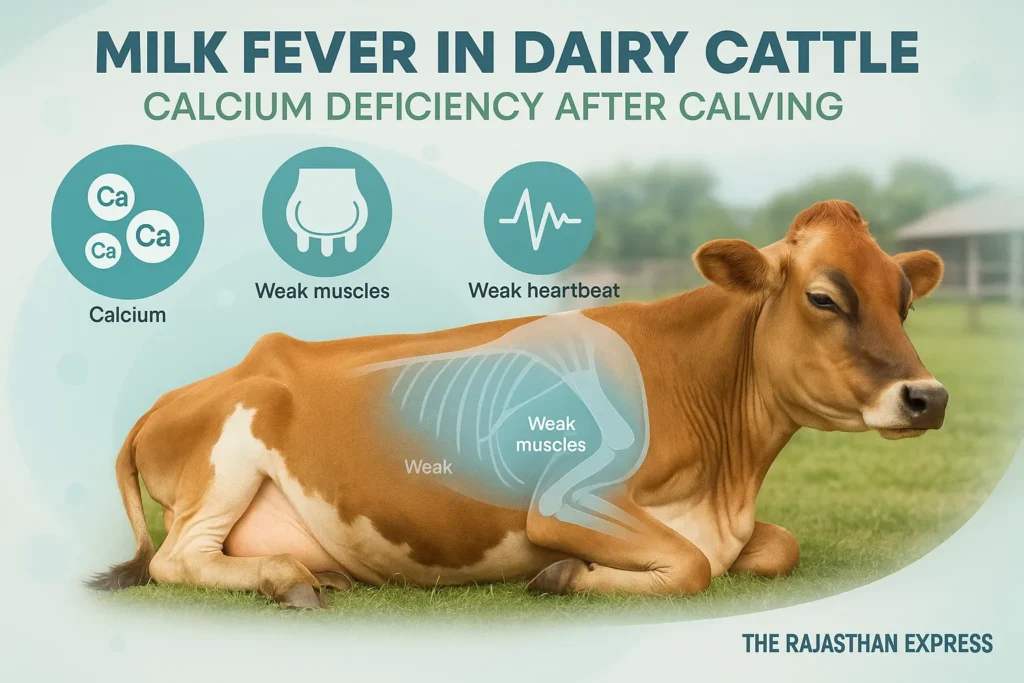
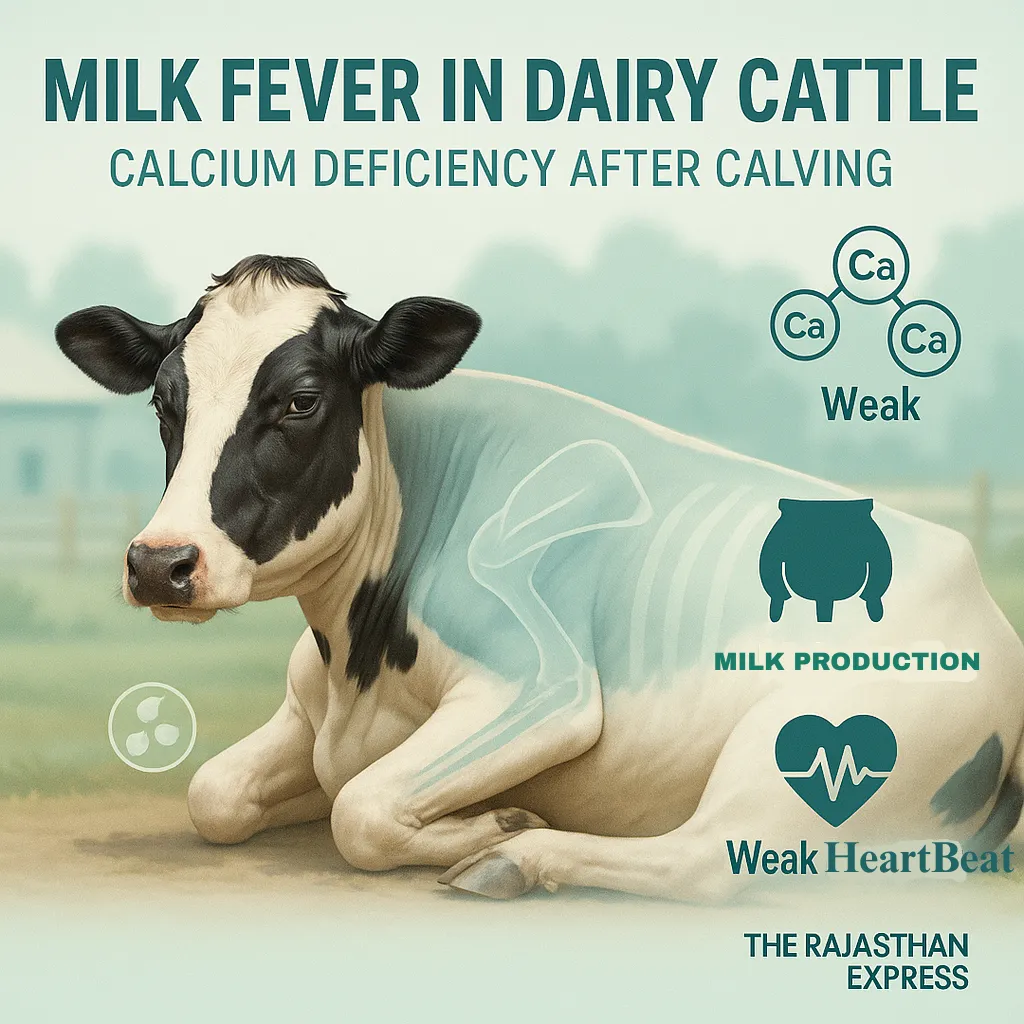
Hypocalcemia causes feverless, flaccid paralysis in the animal. Muscles weaken, blood circulation slows down, and heart rate also decreases.
A specific symptom of milk fever is that the cow sits down by bending its neck towards the flank. This disease usually appears within 72 hours after calving, but in some cases, symptoms may appear 2–3 days before calving.
When the cow starts producing colostrum (first milk), the excretion of calcium from the body exceeds its absorption from the intestines and bones, creating this imbalance.
This disease is observed more in exotic breed cows compared to indigenous cows. It is particularly prevalent in Jersey and Holstein-Friesian breeds.
This disease occurs more in cows than in buffaloes, with the highest likelihood around the third calving; in buffaloes, it is seen more during the fourth calving, while in exotic cows, it is observed more during the fifth calving because milk production peaks at this time.
In dogs, this condition is called Eclampsia.
The normal calcium-to-phosphorus ratio in a cow’s body is 2:1.
Milk Fever (Parturient Paresis) in Dairy Cattle
| Condition | Milk Fever (Hypocalcemia, Parturient Paresis, Puerperal Paresis, Calving Paralysis) |
|---|---|
| Affected Species | Dairy Cattle (cows, buffaloes); rarely seen in small ruminants or dogs (eclampsia) |
| Etiology | Acute calcium deficiency (hypocalcemia) during the peri-parturient period, typically due to sudden demand for calcium during colostrum production exceeding physiological reserves. |
| Typical Onset | Commonly within 24–72 hours post-calving; in some cases, 2–3 days pre-calving. |
| Serum Calcium (Normal) | 8–12 mg/dL (2.0–2.5 mmol/L) |
| Clinical Hypocalcemia Threshold | <5.5 mg/dL; severe cases drop to ~2 mg/dL |
| Most Vulnerable Breeds |
|
| Major Causes |
|
| Common Synonyms |
|
| Clinical Stages & Symptoms |
|
| Pathognomonic Sign | S-bend neck posture (neck bent toward the flank) |
| Diagnosis |
|
| Treatment |
|
| Prevention |
|
| Economic Impact |
|
| Sources: Merck Veterinary Manual, USDA, UMN Extension, Indian Ministry of Fisheries & Dairying, ICAR, The Rajasthan Express | |
Metabolic Disease in Animals: Definition, Types, and Key Characteristics
Definition:
Metabolic Diseases are those diseases which occur due to deficiency, imbalance of nutrients, or disturbance of metabolism in the body. These diseases are especially related to milk production, pregnancy, and the energy requirements of the body.
Read More About : Metabolic Disease
Main Features of Metabolic Disease in Dairy Cattle
- These diseases are Non-Contagious — do not spread from one animal to another.
- In most cases, these diseases are related to the production system, hence they are also called Production Diseases.
- Especially pregnant and milk-producing animals (like cow and buffalo) are more susceptible to these diseases.
- The possibility of metabolic diseases increases with increasing milk production.
- In native cows (Zebu cattle), the highest possibility of metabolic disease is found in the third calving.
- In exotic cows (Exotic Cattle), this possibility is highest in the fifth calving.
- In buffaloes, the possibility of metabolic diseases is mostly in the fourth calving.
- The order of possibility of metabolic diseases is as follows:
Exotic Cow > Native Cow > Buffalo - The possibility of Downer Cow Syndrome, Ketosis, Postpartum Haemoglobinuria, and Mastitis disease is higher in exotic cows, especially in the Holstein-Friesian breed.
- These same diseases are found mostly in the Sahiwal breed in native cows.
- The possibility of Milk Fever is highest in Jersey cows.
We have also explained these diseases in detail.
Explore the key metabolic diseases in cattle with quick links to each section:
- Milk Fever – Calcium deficiency immediately after calving
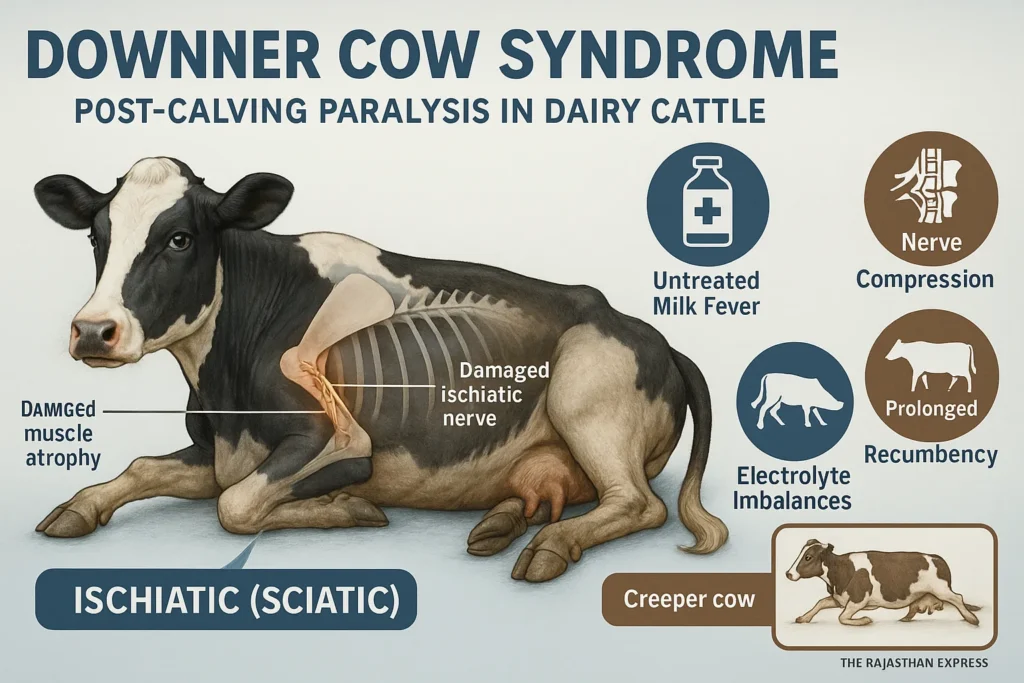
- Downer Cow Syndrome – Complications from prolonged lying after milk fever
- Ketosis In Cattle – Energy deficiency and ketone accumulation
- Postparturient Haemoglobinuria – Red blood cell destruction due to phosphorus deficiency
- Grass Tetany – Muscle cramps from magnesium deficiency
- Pregnancy Toxemia – Energy deficiency in late pregnancy
Blood normally contains:
- Calcium: 8–12 mg / 100 ml
- Phosphorus: 4–8 mg / 100 ml
In milk fever, blood calcium levels drop to about 5 mg below normal, causing acute calcium deficiency in the body.
Key Clinical Signs of Milk Fever
- Characteristic S-bend posture: Neck bent toward flank
- Onset: Within 72hrs post-calving (or 2-3 days pre-calving)
- Triad of symptoms:
» Muscle weakness
» Slowed circulation
» Reduced heart rate
Breed Vulnerability of Milk Fevar
| Breed Vulnerability of Milk Fever | ||
| Species | Peak Occurrence | Risk Level |
|---|---|---|
| Exotic Cows | 5th calving | ★★★ (Highest) |
| Indigenous Cows | 3rd calving | ★★☆ |
| Buffaloes | 4th calving | ★☆☆ |
| High-risk breeds: Jersey, Holstein-Friesian | ||
| Breed Vulnerability of Milk Fever : The Rajasthan Express | ||
Main Causes of Calcium Deficiency
- Excessive excretion of calcium through colostrum.
- In rural areas, additional suckling by the calf after feeding colostrum further increases calcium deficiency in the body.
- Lack of mineral mixture or balanced diet during pregnancy.
Synonyms and Alternate Names for Milk Fever
| Synonyms and Alternate Names for Milk Fever | |
| English Name | Meaning / Explanation |
|---|---|
| Milk Fever | Acute calcium deficiency disorder in cows or buffaloes during calving. |
| Parturient Paresis | Loss of muscle function after calving. |
| Hypocalcemia | Blood calcium level falls below the normal range. |
| Puerperal Paresis | Muscle weakness during or after parturition (delivery). |
| Parturient Apoplexy | Sudden paralysis due to brain or nerve dysfunction around the time of calving. |
| Calving Paralysis | Paralysis caused by nerve damage or pressure during the calving process. |
| Synonyms and Alternate Names for Milk Fever : The Rajasthan Express | |
📌 Note:
- Both Calving Paralysis and Milk Fever occur around calving.
- In Stage 3 of Milk Fever, prolonged lying on one side may compress/injure nerves, leading to Calving Paralysis.
Key Similarities in Livestock Disorders
- Milk Fever occurs most within 72 hours post-calving in cows.
- Similarly, Colibacillosis (Calf Scour/White Yellow Diarrhea) is observed in newborn calves, lambs, piglets, foals, and kids within 72 hours of birth.
Predisposing Factors
- Dietary calcium deficiency
- High milk production
- Unavailability/irregularity of mineral mixtures
Milk Fever Symptoms and Clinical Stages
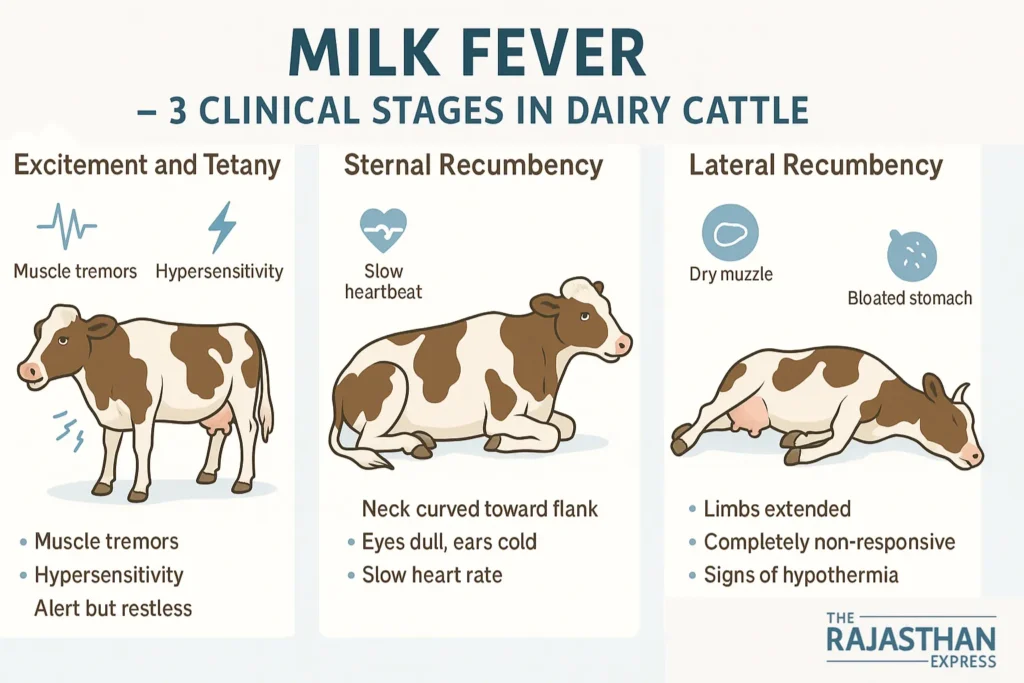
Milk fever symptoms are divided into three stages:
Stage 1: Initial Excitement and Tetany
- Muscle tremors, especially in the head and legs
- Hypersensitivity
- Body temperature slightly above normal
- Animal stops eating, appears dull
- Head shaking, protrusion of tongue
- Teeth grinding, restlessness
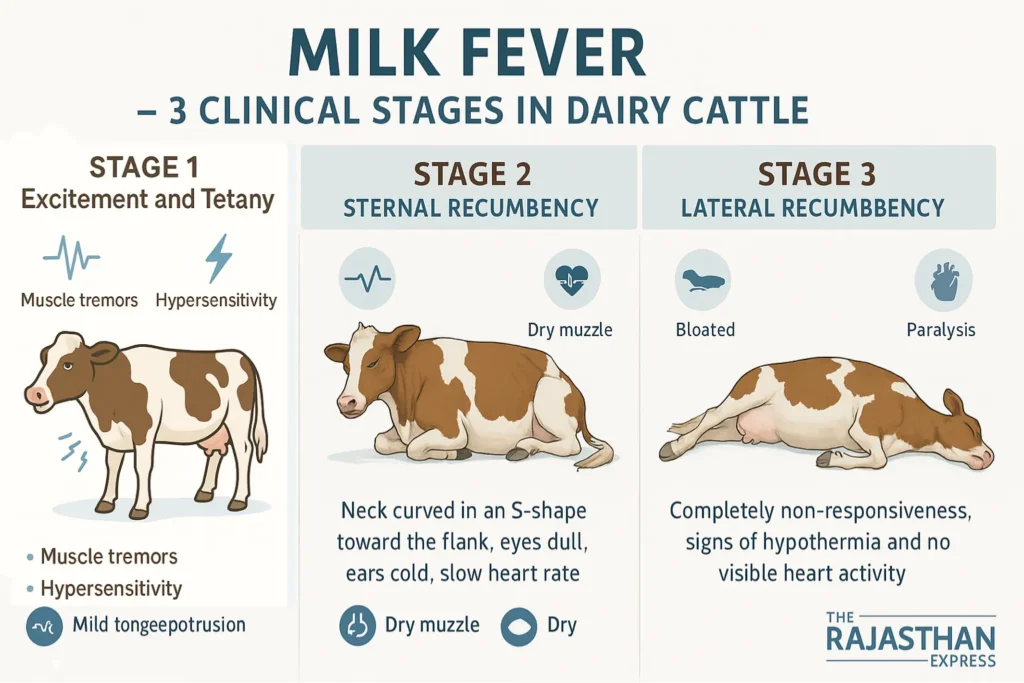
Stage 2: Flaccidity and Sternal Recumbency
- Cow lies on its belly or remains seated on the sternum
- Neck bent towards the flank (Kinking of Neck or S-Shape Posture)
- Dry muzzle, cold skin and limbs
- Low body temperature (Hypothermia)
- Slow heartbeat (~80 per minute)
- Rumination stops, gas formation and constipation
- Difficulty or slowness in urination
Stage 3: Critical Condition (Lateral Recumbency)
- Cow lies on one side, fully stretched out
- Limbs flaccid, no response when moved
- Animal is almost unconscious
- Very low body temperature
- Heartbeat inaudible (Heart Sound Absent)
- Unable to change position independently
Milk Fever Diagnosis Methods
History-Based Clues
- Inability of cow/buffalo to stand immediately after calving
- Excessive colostrum loss, especially after residual milk is extracted post calf-feeding (colostrum contains 10–12 times more calcium than normal milk)
- Kinking of Neck, low body temperature, and lateral recumbency
Blood Test
- Blood calcium level drops below 5 mg/dl (down to 2 mg/dl in severe cases).
Sulkowitch Test (Urine Test)
- Used to detect calcium presence in urine.
Differential Diagnosis: Milk Fever vs. Similar Conditions
Conditions with similar symptoms include:
- Hypophosphatemia (Phosphorus deficiency)
- Hypomagnesemia (Magnesium deficiency)
- Downer Cow Syndrome
- Fat Cow Syndrome
- Excessive carbohydrate intake
- Acute Coliform Mastitis
- Aspiration Pneumonia
- Severe gastrointestinal inflammation
- Spinal Cord Injury
- Hip Joint Luxation (dislocation)
Milk Fever Treatment Protocol
Primary Drug: Calcium Borogluconate (CBG)
- 23% or 25% solution
- 450 ml dose:
- 250 ml slow intravenous (IV)
- 200 ml subcutaneous (SC)
- Small animals: 50–100 ml
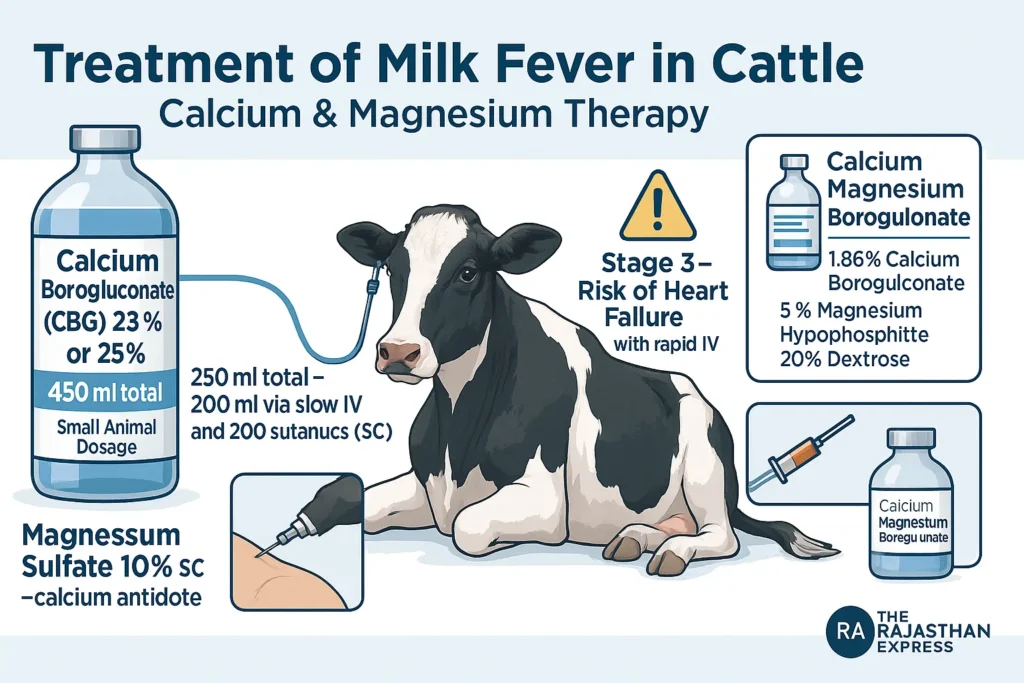
Precautions
- Rapid IV drip in Stage 3 may cause dangerously increased heart rate leading to heart failure.
- Administer 10% Magnesium Sulfate SC simultaneously (magnesium acts as calcium’s antidote).
Combined Deficiency Solution
For concurrent calcium, phosphorus, and magnesium deficiency:
- Calcium Magnesium Borogluconate contains:
- 1.86% Calcium Borogluconate
- 5% Magnesium Hypophosphite
- 20% Dextrose
- Dose:
- 450–800 ml (large animals)
- 50–100 ml (small animals) IV
- Repeat after 10–12 hours if needed.
Heart Monitoring
- Monitor heartbeat during treatment.
- Stop IV immediately if abnormal rhythm (slow/fast/irregular).
- Administer Antihistamine (Pheniramine Maleate): 1–2 mg/kg IM.
Milk Fever Prevention and Control
- Implement balanced dietary management during pregnancy and calving.
- Ensure adequate calcium, phosphorus, and magnesium in feed.
- Supplement Vitamin D for proper intestinal calcium absorption.
DCAD (Dietary Cation-Anion Difference)
- Maintain pre-calving DCAD at 50–150 meq/kg.
- Use anionic salts twice weekly:
- Calcium Chloride
- Magnesium Chloride
- Calcium Sulphate
- Magnesium Sulphate
Difference Between Milk fever and Downer Cow Syndrome
| Difference Between Milk fever and Downer Cow Syndrome : The Rajasthan Express | ||
| Parameter | Milk Fever (Hypocalcemia) | Downer Cow Syndrome (DCS) |
|---|---|---|
| Definition | Acute calcium deficiency (<5.5 mg/dL) due to excessive calcium loss in colostrum. | Secondary complication from prolonged recumbency (>24 hours), often following untreated milk fever, causing nerve/muscle damage. |
| Primary Cause | Sudden calcium demand for colostrum production exceeding mobilization capacity. | Untreated milk fever, trauma during calving, or electrolyte imbalances (Ca, P, Mg, K) leading to sciatic nerve damage. |
| Onset | Within 72 hours post-calving (occasionally 2–3 days pre-calving). | Develops 2–3 days post-calving after prolonged recumbency (>24 hours). |
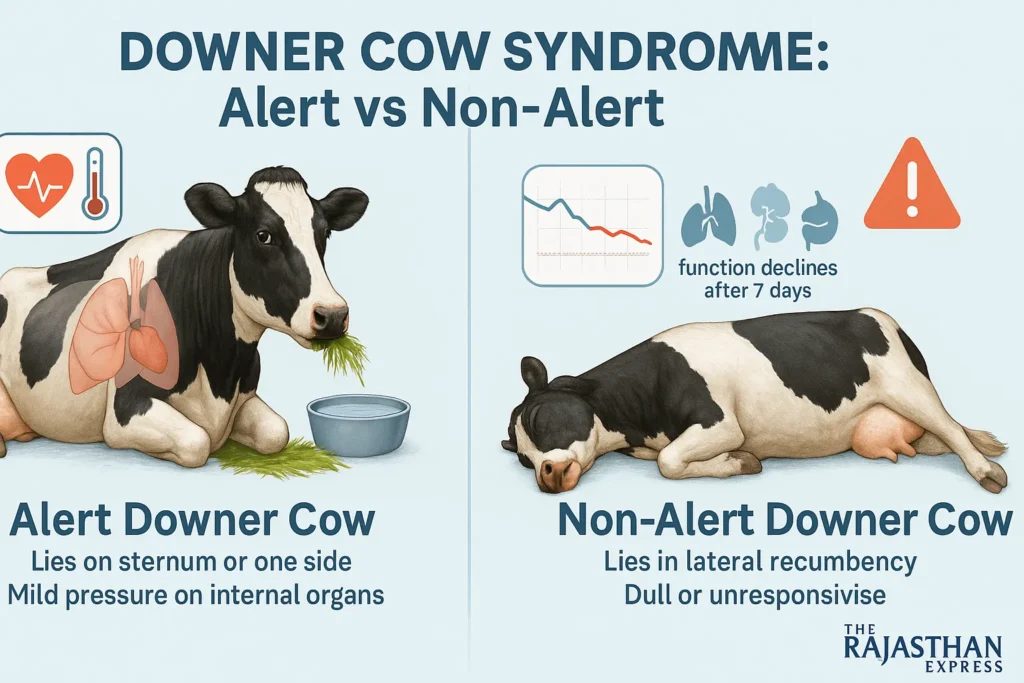
| Key Clinical Signs |
Stage 1: Muscle tremors, restlessness. Stage 2: Sternal recumbency, “S-bend neck,” hypothermia. Stage 3: Lateral recumbency, coma. |
Alert DCS: Eats/drinks normally but cannot stand. Creeper Cow: Crawls using forelimbs. Non-alert DCS: Coma, organ failure. |
| Diagnosis |
– Blood Ca²⁺ <5 mg/dL. – Sulkowitch urine test (low calcium). – Clinical signs (e.g., “S-bend neck”). |
– Elevated CPK (>1000 IU/L) and AST (>500 IU/L). – History of dystocia or untreated milk fever. – Myoglobinuria (brown urine). |
| Treatment | IV 23% calcium borogluconate (250 mL IV + 200 mL SC). Supportive: Magnesium sulfate SC to prevent tetany. |
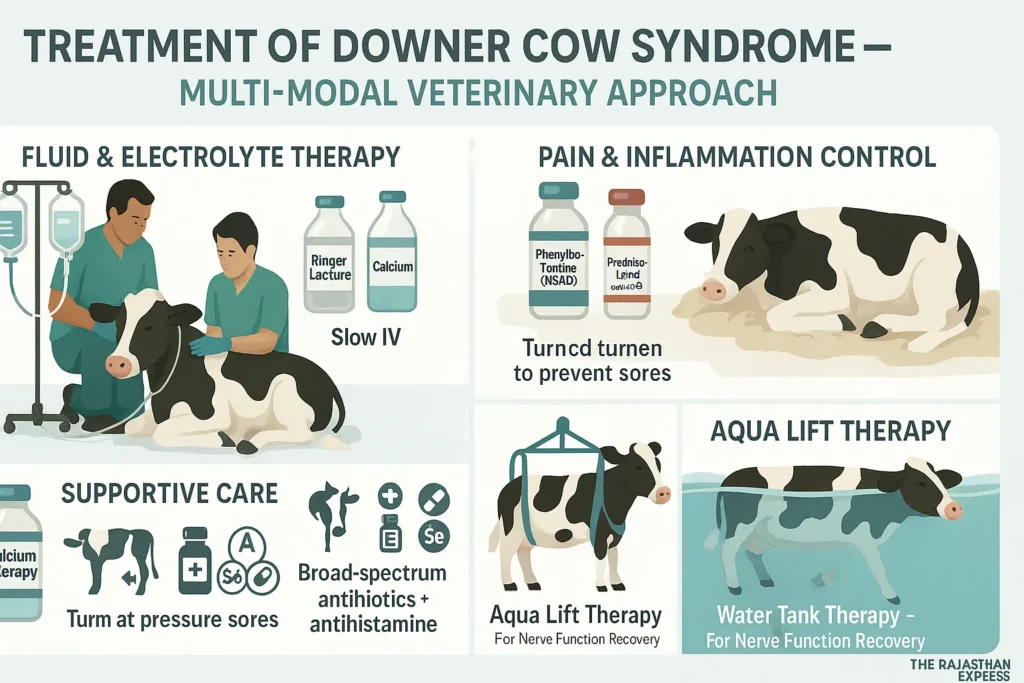
Multimodal: – Electrolyte fluids (Ca, Mg, P). – NSAIDs (phenylbutazone). – Nursing care (slings, side rotations). – Aqua lift therapy. |
| Breeds at Risk | Jersey > Holstein > Exotic breeds (peak at 5th lactation). | Holstein-Friesian (5th lactation) > Buffaloes. |
| Prevention | DCAD diets pre-calving (anionic salts). Oral calcium boluses at calving. Vitamin D₃ supplementation. |
Prompt milk fever treatment (within 4–6 hours). Soft bedding to avoid pressure injuries. Avoid over-conditioning pre-calving. |
| Prognosis | Excellent if treated early (90% recovery). | Guarded (30–50% recovery if recumbent >7 days). |
| Economic Impact | $334/case (milk loss, treatment costs). | >$1000/case (extended care, culling). |
| Key Pathophysiological Differences | ||
| Mechanism of Recumbency | Flaccid paralysis due to hypocalcemia impairing neuromuscular function. | Ischemic muscle/nerve damage (sciatic compression) from prolonged recumbency. |
| Electrolyte Involvement | Primarily calcium deficiency (Ca²⁺ <1.6 mmol/L). | Multifactorial: Ca, P, Mg, K deficiencies + muscle enzyme leaks (CPK/AST). |
| Response to Treatment | Rapid improvement post-calcium infusion (stands within 1–2 hours). | Requires days of rehabilitation; success depends on early intervention. |
| Difference Between Milk fever and Downer Cow Syndrome : The Rajasthan Express | ||
Read More About : Downer Cow Syndrome
Stop milk fever losses! Learn proven DCAD diets, IV protocols & breed-specific prevention for dairy cows. Includes subclinical risks, relapse fixes, and buffalo/cattle differences. Trusted by vets.
THE RAJASTHAN EXPRESS
Frequently Asked Questions About Milk Fever in Cows
Why do some cows with normal calcium levels still show milk fever symptoms?
- Ionized calcium deficiency: Only ionized calcium (iCa) supports neuromuscular function; acidosis or alkalosis can reduce iCa despite normal total calcium.
- Hypomagnesemia: Low magnesium impairs parathyroid hormone (PTH) release, hindering calcium mobilization.
- Electrolyte imbalances: Elevated potassium or phosphorus decreases calcium absorption and PTH sensitivity.
- Example: A cow with total calcium at 8.0 mg/dL but iCa < 1.0 mmol/L may still be recumbent due to functional hypocalcemia.
How to practically implement and monitor DCAD diets for milk fever prevention?
Implementation:
- Formula: DCAD (mEq/kg DM) = (Na⁺ + K⁺) – (Cl⁻ + S²⁻)
- Target: -100 to -200 mEq/kg for prepartum cows (21 days before calving)
- Use anionic salts (e.g., CaCl₂, MgSO₄) in TMR to improve intake
Monitoring:
- Urine pH weekly: Ideal 5.8–6.8 (Holsteins), 6.0–6.5 (Jerseys). pH >7.0 = inadequate acidification
- Forage testing: High-potassium forages compromise DCAD diets
- Tip: Avoid feeding anionic diets >3 weeks pre-calving to prevent reduced intake
Why are Jersey cows more susceptible to milk fever than Holsteins?
- Fewer vitamin D receptors: 95 vs. 142 fmol/mg in Holsteins, impairing calcium absorption
- Higher milk yield per kg body weight: 31.7 vs. 35 kg/day increases calcium loss
- Age factor: 24.85% incidence after 4th parity in Jerseys vs. 8.29% in Holsteins
Can oral calcium boluses worsen milk fever relapse rates?
- Yes, if misused: Boluses given to normocalcemic cows suppress PTH response, increasing relapse risk
- Targeted use only: Effective in high-risk cows (≥3 lactations, history of hypocalcemia)
- Benefit: 50–60% relapse reduction post-IV treatment; lame cows had 0.34 fewer health events
What are the long-term impacts of subclinical hypocalcemia on reproduction and immunity?
Reproduction:
- Extended calving intervals by 15–30 days
- 1.5–2× more inseminations per pregnancy
Immunity:
- 20–30% higher somatic cell counts
- 1.8× higher clinical mastitis incidence
- Cost: €54 per cow in treatment and yield loss
Is udder inflation a valid milk fever treatment today?
- No: Obsolete and hazardous method
- Risks: Introduces mastitis, causes stress, fails to correct hypocalcemia
- Current standard: IV calcium borogluconate (23%) + oral calcium for sustained effect
Why does IV calcium increase relapse risk in downer cows?
- Rebound hypocalcemia: IV surge suppresses PTH, hindering calcium regulation
- Cardiac risks: Rapid infusion may cause arrhythmias
- Recommended protocol: 250 ml IV slow drip + 200 ml SC + oral bolus
How does milk fever differ in buffalo versus cattle?
- Lower susceptibility: More efficient bone calcium mobilization
- Lower milk per body weight: Reduces calcium drain
- Peak incidence: At 4th calving vs. 3rd (indigenous cows) or 5th (Holsteins)
What role does hypomagnesemia play in milk fever non-response?
- Essential for PTH function: Mg < 1.8 mg/dL blunts PTH release
- Failure to respond: Seen in 15–20% of treated cows without Mg correction
- Solution: Supplement 10% MgSO₄ subcutaneously
Can high-potassium forages cause milk fever in beef cows?
- Yes, though less common: High-K forages (e.g., alfalfa) cause positive DCAD → metabolic alkalosis
- At-risk: Older, beef-dairy cross cows with high milk yield
- Prevention: Use low-K forages (grass hay) or add anionic salts